
Treatment of anal fistulas with radiofrequency
What is a fistula?
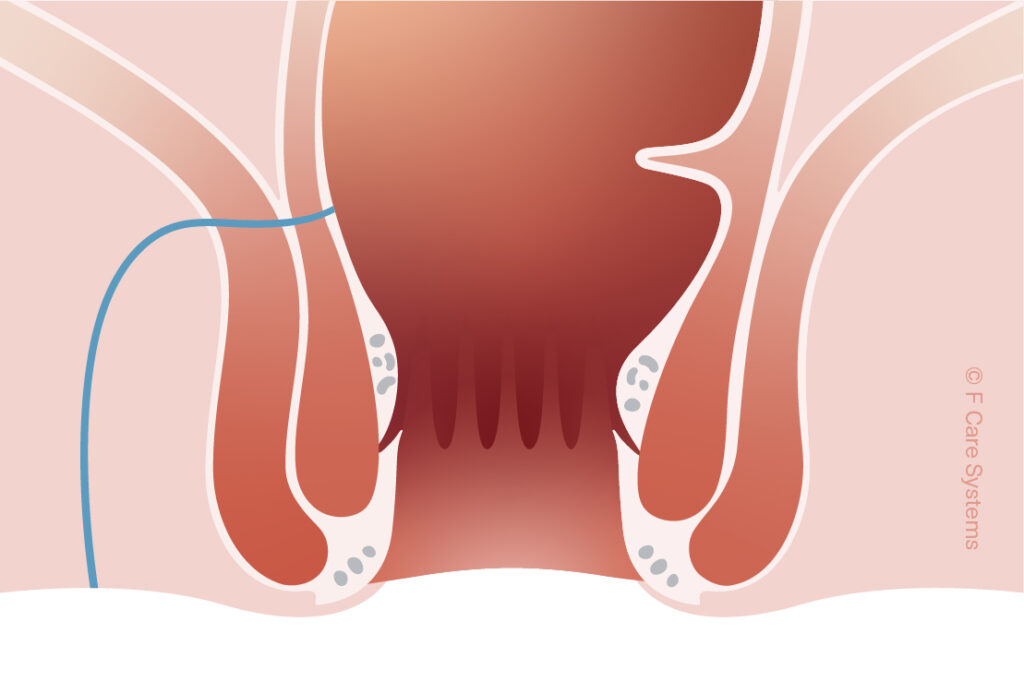
A fistula (Latin for “tube” or “pipe”) is any abnormal connection between two body parts that aren’t normally linked, such as two organs, two blood vessels (i.e., an artery and a vein), or an internal organ and the surface of the skin. Some people are born with fistulas; others develop them in connection with injuries, illness, or certain medical treatments. The most common type of fistula is the fistula-in-ano, or anal fistula, which connects the rectum to the skin near the anus.
What causes anal fistulas?
Anal fistulas, also known as fistula-in-ano,are usually the result of an abscessed (clogged and infected) gland in the anus, because pus collects in the surrounding tissue and forms a small channel as it drains away. They can also occur due to inflammation of the digestive tract, for example due to Crohn’s disease or ulcerative colitis.
Researchers aren’t entirely sure why some people develop anal fistulas and others don’t, but the important thing to know is that they’re caused by inflammation, not poor hygiene. They are most common in adults around the age of 40, but they can occur in younger people as well, especially those with a history of chronic digestive issues. Other potential risk factors for anal fistulas include:
- Previous history of anal abscess or fistula
- Trauma (injury) to the area
- Previous surgery or radiation therapy
- Certain infections, such as tuberculosis or HIV
- Diabetes
Types of anal fistulas
Anal fistulas are classified by location, and by which of the sphincter muscles (the ones used to control bowel movements) are involved. In order from most to least common, the four types are:
- Intersphincteric (between the internal and external sphincter muscles)
- Transsphincteric (passing through both sphincter muscles)
- Suprasphincteric (circling up and over the external sphincter muscle)
- Extrasphincteric (around the outside of the sphincter muscles)



How do I know if I have an anal fistula?
Since anal fistulas typically form due to drainage, one common symptom is pus or other fluid leaking near the anus, which may have an unpleasant odor and cause itching or irritation. Other possible symptoms include:
- Swelling and redness in your anal area
- Throbbing pain that gets worse when you move around, sit down, cough, or use the toilet
- Fever, chills, feeling sick in general
- Blood or pus in stool
- Bowel incontinence in some cases
Preventing anal fistulas
You can reduce your risk of anal fistulas by avoiding constipation, for example by eating a fibre-rich diet and drinking plenty of water. Getting regular exercise will also help you keep your stools soft and your bowels working properly. Make sure to use the toilet as soon as you feel the urge, and keep your bottom clean and dry—even though fistulas and personal hygiene aren’t directly linked, cleanliness can reduce your risk of skin infections. Sitting for long periods of time may also increase the risk of fistulas in people already predisposed to them; try sitting on a donut pillow to reduce the pressure on your back and lower body.
Anal fistula treatment with Fistura®
If you suspect you may have a fistula-in-ano, it’s important to seek medical attention—even if the underlying abscess (infection) clears up, the fistula itself is unlikely to heal on its own, and it could cause additional infections if left untreated. If your GP suspects you have a fistula, he or she can refer you to a colorectal specialist for additional tests and treatment.
Although fistulas are often treated with surgery (by cutting along the length of the fistula so that it leaves a flat scar), the procedure can require several weeks or even months of painful recovery, and carries a risk of anal incontinence.
One new sphincter-saving option is Fistura®, a procedure that ablates (= removes) the fistula using radio waves. The doctor inserts a thin, flexible catheter into the fistula and applies targeted radiofrequency energy at the tip of this catheter; the resulting heat destroys the walls of the fistula tract while leaving the surrounding healthy tissue intact. The catheter is slowly drawn back through the fistula, sealing the fistula little by little.
Advantages of Fistura®
- Performed as a day case – takes just a few minutes
- Minimally invasive (no incision), which means no risk of incontinence
- Little to no pain; minimal after-care
- Suitable for treating Crohn’s-related fistulas
- Resume normal daily activities quickly